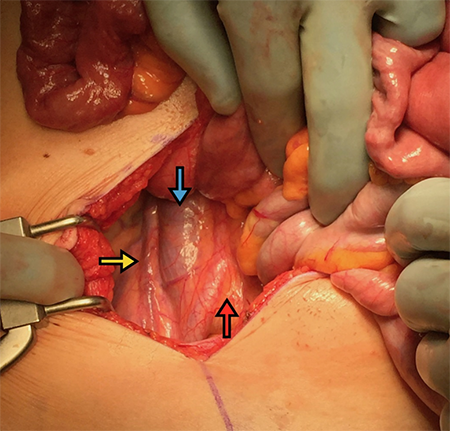
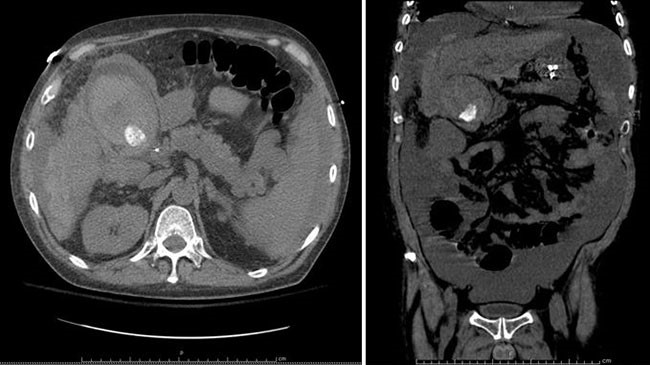
Figure 6. The duodenum (D) does not cross midline, with the head of the pancreas (P) readily visible and protuberant out from the retroperitoneum.
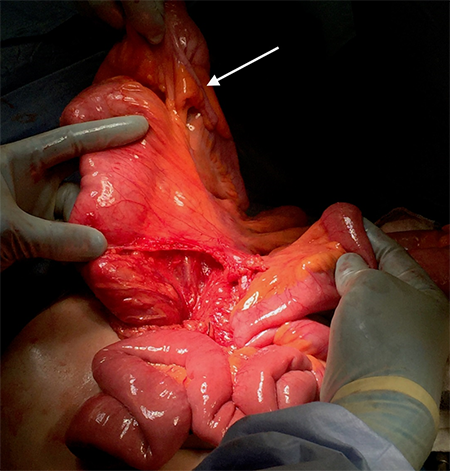
The small intestine was detorsed in a counterclockwise direction, the abnormal fibro-fatty bands were lysed, the duodenum was mobilized as much as possible, an appendectomy was performed, and the bowel was examined for viability before being returning the small bowel to the right hemiabdomen and the cecum to the left upper quadrant.
Postoperatively the patient’s presenting pain was absent and she was discharged after regaining bowel function without incident. At one-month follow-up, the patient was free of her prior symptoms of intermittent crampy abdominal pain and was doing well.
Discussion
CIM is a spectrum of anomalies affecting the development and rotation of the gastrointestinal tract. Typically considered a malady of infancy, of the 0.2% incidence of live births, an estimated 75 percent of cases are identified within the first year of life. Malrotation predisposes affected infants to acute midgut volvulus, which is frequently how they present. This is characterized by sudden-onset bilious emesis with eventual intestinal ischemia, and accompanying mortality rates of up to 24 percent.1
The etiology of CIM lies in errors of embryologic development. Normal intestinal rotation happens as a three-stage process, where the nascent intestinal tract begins as a single loop—with the superior mesenteric artery (SMA) as the center axis. The cranial aspect of the loop is termed the duodenojejunal (D-J) loop, and the caudal referred to as the cecocolic (C-C) loop. The result of this process in normal anatomy is a 270° counter-clockwise turn of both loops, essentially opposite one another, around the SMA axis. It is important to note, however, that malrotation can manifest as various permutations of complete, partial, or nonrotation of either or both of the D-J and C-C loops. Balthazar described six subtypes (radiographically) of such combinations, noting that normal rotation of one loop does not exclude malrotation in the other.2
CIM presenting in the adult is quite rare and is typically a much more difficult process to diagnose than in infancy. Assessment of true incidence of CIM in adulthood is precluded by the lack of symptoms and subsequent presentation in a significant proportion of patients. Reported presentations are typically quite similar to the patient presented hereyears of episodic nonspecific symptoms, including crampy abdominal pain, nausea, and constipation. Often, multiple past CT scans are read out as normal, and such patients frequently have been subjected to misguided operations that tried and failed to cure their pain (e.g., cholecystectomy).3 These symptoms can usually be attributed to congenital adhesive bands associated with CIM or a chronic midgut volvulus. A second form of adult presentation is with acute-onset obstruction and pain, caused by an acute volvulus.4
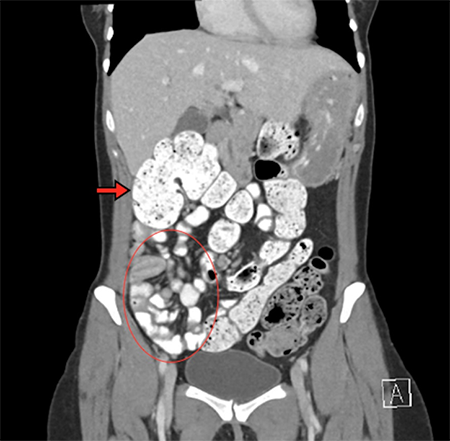
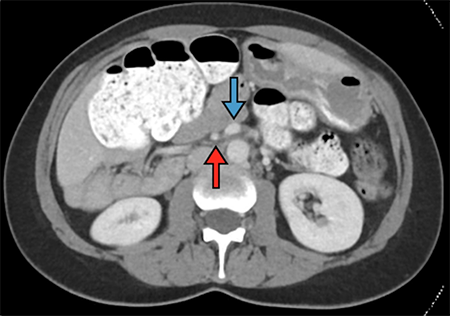
Diagnosis is secured by either contrasted upper gastrointestinal series or abdominal CT. The former demonstrates a lack of crossing of the midline by the duodenum, while the latter shows small bowel clustered on the right side of the abdomen and the SMV located to the left of the SMA. Surgical intervention with laparotomy and the Ladd procedure has been the standard of care since Ladd described it in 1932.
5This includes division of Ladd bands (from cecum to the right abdominal wall), division of mesenteric bands, reduction of volvulus, appendectomy, and placement of the small bowel on the right side and colon on the left side of the abdomen.
Conclusion
Experiencing lifelong symptoms of intermittent abdominal pain along with prior radiographic examinations read out as “normal” emphasizes that although CIM with midgut volvulus is an infrequent cause of abdominal pain in adults, it should remain in the differential when the etiology of pain is uncertain, especially in those without past abdominal surgical history.
Lessons Learned
CIM is frequently associated with a delay in diagnosis when presenting in adulthood and often attributed to other nonspecific causes. Patients can present with acute midgut volvulus mandating emergency surgery. Awareness of the variations of anatomical malrotation as well as presentation, radiographic findings, and surgical principles are vital to ensure accurate and timely diagnosis and intervention.
Authors
Deschner BW, Schwulst SJ
Correspondence Author
Benjamin W. Deschner, MD
927 W Wrightwood Ave, Unit A
Chicago, IL 60614
Author Affiliations
Northwestern University
Department of Surgery
Division of Trauma and Critical Care
676 N. St. Clair St., Ste #650
Chicago, IL, 60611
References
- Al-Salem, AH. Intestinal Malrotation. In: An Illustrated Guide to Pediatric Surgery. Cham: Springer International Publishing; 2014: 173-180.
- Balthazar, EJ. Intestinal malrotation in adults. Roentgenographic assessment with emphasis on isolated complete and partial nonrotations. Am J Roentgenol. 1976; 126(2):358-367.
- Gamblin, TC, Stephens RE, Johnson RK, Rothwell M. Adult malrotation: a case report and review of the literature. Curr Surg. 2003;60(5):517-520.
- Dietz, DW, Walsh RM, Grundfest-Broniatowski S, Lavery IC, Fazio VW, Vogt DP. Intestinal malrotation: a rare but important cause of bowel obstruction in adults. Dis Colon Rectum. 2002;45(10):1381-1386.
- Ladd WE. Congenital obstruction of the duodenum in children. N Engl J Med. 1932;(206):277.