Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Effective Intraoperative Teaching: From Theory to Practice
Jordan D. Wood, MD; V. Prasad Poola, MBBS, FACS; John D. Mellinger, MD, FACS
July 1, 2020
20 MinPrintShare
Bookmark
Figure 1: Zone of Proximal Development (Orange Zone)
Intraoperative teaching and learning shapes the fundamental and essential core competency of a surgeon: operative skills. For a variety of well-documented reasons—including a duty hour-compressed learning paradigm, minimally invasive trends, regulatory pressures, and fiscal and quality performance expectations—the opportunity for resident operative autonomy1 and related preparedness and self- confidence for independent practice has diminished.2 Improving the quality of intraoperative teaching and learning is a critical educational strategy in the current surgical training environment. Despite mandates for and the proliferation of simulation and skill centers, the operating room remains the predominant venue in which trainees advance and demonstrate autonomous technical skill and sound operative judgment. In fact, while all accredited institutions now have some form of skill development laboratory, many lack an organized strategy focused on maximizing teaching and learning in the setting of the operating room itself. The purpose of this article is to provide a succinct and evidence-based framework for enhancing operative teaching and learning. The model presented is based on the prior work of Roberts et al at our institution, namely the BID Model (briefing, intraoperative teaching, and debriefing).3
Briefing: Know Your Learner
A brief interaction with the trainee prior to entering the operating room is an essential first step. Without it, an opportunity for setting and agreeing on the goals and expectations for both teacher and learner is lost. This interaction helps the attending to gauge the trainee’s preparedness and prior experience with the procedure, provides an opportunity to review the operative steps, and identifies the gaps in the trainee’s knowledge of operative sequence, maneuvers, and instrument requirements. Ideally, this preoperative briefing should occur in a relaxed and focused setting, such as the surgical lounge. However, it can be done meaningfully in a very succinct amount of time (2–5 minutes), while the attending and resident are scrubbing together for the procedure (the “scrub sink classroom”). Encouraging residents to think through the steps of a procedure preoperatively has been shown to improve the opportunity for early autonomy during the operation. More organized and deliberate forms of preoperative goal setting, such as the “educational time-out” can also be employed to amplify resident engagement in pre-operative goal setting, and to improve autonomy in the operating room.4
Intervention in the Operating Room: Provide Scaffolded Autonomy
Providing progressive autonomy or entrustment in the operating room is perhaps the most critical factor in preparing the resident for confident, independent practice. Autonomy is elusive to detail with definitive clarity, for reasons including significant differences in perception between residents and faculty surgeons.5,6 An effective preoperative briefing discussion may help to mitigate some of these perceptional issues and improve autonomy.4 Though challenging, providing opportunities to struggle and learn is the ultimate responsibility of the faculty surgeon and must be done while maintaining patient safety and fiscal efficiency. Familiarity with Vygotsky’s concept of the “zone of proximal development” (see Figure 1)—which provides a framework for the focus and next step orientation in the transition of junior to senior learner in any given teaching interaction by navigating through the “interplays between student regulation and teacher regulation of the learning process”—is an exceptionally helpful construct. The faculty surgeon in this framework orients their teaching effort to whatever element(s) of the operative sequence can be performed by the learner with their assistance but could not be performed without it. This allows the teaching focus of the case to be efficiently oriented to the point of greatest benefit for the learner and creates a structure for appropriately facilitated autonomy. The trainee thereby can progress from known to unknown in a safe and focused fashion, moving through the zones of proximal development—in other words, those areas that represent true next step elements in their own specific skill progression. If an isolated or more general technical deficiency is noted, such as knot tying or unfamiliarity with the use of a specific instrument, it may be identified and then remediated or addressed in a safe and less time-pressured simulation setting, especially for junior or midlevel residents.
Figure 1: Zone of Proximal Development (Orange Zone)
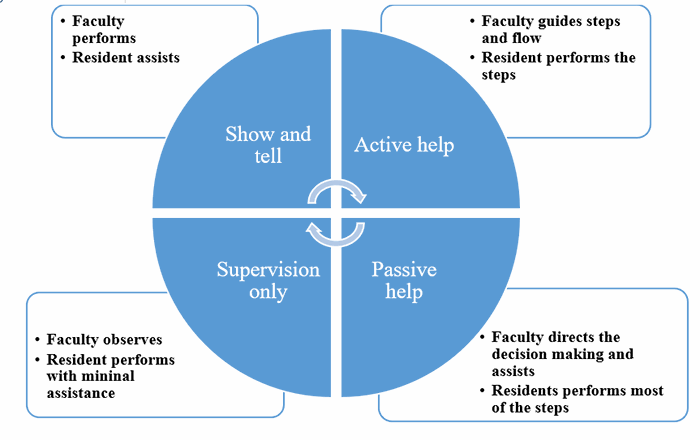
Figure 2: Zwisch scale
Teaching nontechnical skills such as situational awareness, decision making, communication, teamwork, judgment and leadership in the operating room is just as important, if not more so in some respects, than educating on technical skills.7 The resident’s ability to set up the operating room, anticipate next steps, communicate effectively with the OR staff, and consciously slow down during a critical portion of the procedure are skills best taught by role modeling progressing to entrustment and observed autonomy in the OR. At the same time, this learning can be leveraged or augmented by simulation or didactic teaching strategies.8 Proficiency with these non-technical skills leads to a confident and competent surgeon, and deficiency in such skills has been shown to be detrimental to patient safety.9,10
Debriefing: Ask Trainee What They Have Learned
Debriefing after a procedure is essential to optimize the learning opportunity. It is most effective if conducted immediately after the procedure, before recall difficulties arise, while the experience is fresh and still being processed by the learner.11 This allows the resident to assess their own performance and provide feedback both to the teacher and themselves. Debriefing is most effective when conducted by sit-down interview, allowing the resident to review each step of the procedure critically as a means of reinforcing sequencing and operative flow. Given contemporary time constrains, it can be accomplished in a more limited time, such as during skin closure or while placing postoperative orders, ensuring convenient integration into the necessary existing workflow.3
An effective debriefing should be nonjudgmental but honest, identifying both positive and negative aspects of performance. It should focus on specifics and provide detailed steps for future improvement.11 It is important to engage the learner in an open-ended discussion by asking questions such as “How do you think that went?”, “What did you learn that was new?”, and “What would you do differently next time?” Unfortunately, debriefing is underutilized by faculty surgeons and provides the greatest opportunity to improve teaching impact. The use of structured evaluation tools such as OPRs, SIMPL, or other performance scales (see below) can provide a shared template for conducting the debriefing and creating an enduring record for future learning reference. Creating a culture that emphasizes the uniform need for debriefing will help to maximize its utilization and impact.11
Evaluation: Provide Structured Assessment
Assessment of single performance events for a resident by a faculty surgeon over a period of time has proven more informative, granular, and meaningful when compared to summative assessment of operative skills at the end of a month-long surgical rotation.12 Such assessments, even at a rate of two to three per month, provide objectivity and validation of resident operative performance trajectory, particularly when performed by a range of faculty to minimize evaluator bias. Such assessments can also be used in providing summative feedback and guiding decisions regarding remediation or promotion of a trainees.13,14
The Zwisch scale (see Figure 2) provides a simple metric for guiding and grading the progression towards autonomy in four stages: Show and tell, Active help, Passive help, and Supervision only.15 Based on the principles of the Zwisch scale, the Procedural Autonomy and Supervision System (PASS) and System for Improving and Measuring Procedural Learning (SIMPL) proficiency scales are both attested and easily accessible tools. Both PASS and SIMPL are user friendly and are available via mobile app platforms to facilitate temporally proximate utilization by the faculty surgeon and resident.16
Figure 2. Zwick Scale
Step
Objective
1
Briefing
Setting the goals and objectives
2
Guided autonomy
Provide autonomy in both technical and non-technical skills
3
Debriefing
Allow reflection and enhance insight
4
Evaluate
Aid to resident technical skills trajectory
The above outline provides a technical framework for intraoperative teaching in a time-pressured environment where every opportunity counts. Importantly, resident perception and reception of operative teaching is strongly associated with surgeons who demonstrate positive attitudes towards teaching, and remain calm and courteous in the operating room.17 If one can make an argument that intraoperative teaching is a skill, then it could be mastered by deliberate practice, aiming towards achieving the balance between patient-centered care and learner-centered education, one resident and one case at a time. Faculty development by a half-day course or similar strategies, in which the principles of intraoperative teaching are outlined and rehearsed, is an effective strategy in educating and implementing these principles.18
Summary
Strategies to improve intraoperative teaching are critical in the current training paradigm in which technical skill development is pressured by time, productivity, and regulatory pressures. Disciplined use of structures to enhance operative teaching, such as the BID model and scales focused on evaluating and leveraging autonomy, can be employed as simple, targeted and effective strategies to enhance learning in the operative setting. Programs that intentionally develop habits in using such strategies will optimize the educational impact of each operative learning opportunity for their trainees.
References
Hashimoto, D.A., et al., See More, Do More, Teach More: Surgical Resident Autonomy and the Transition to Independent Practice. Acad Med, 2016. 91(6): p. 757-60.
Scally, C.P., et al., Investigating the Impact of the 2011 ACGME Resident Duty Hour Regulations on Surgical Residency Programs: The Program Director Perspective. J Am Coll Surg, 2015. 221(4): p. 883-9 e1.
Roberts, N.K., et al., The briefing, intraoperative teaching, debriefing model for teaching in the operating room. J Am Coll Surg, 2009. 208(2): p. 299-303.
Lillemoe, H.A., et al., A Preoperative Educational Time-Out is Associated with Improved Resident Goal Setting and Strengthens Educational Experiences. J Surg Educ, 2020. 77(1): p. 18-26.
Rose, J.S., B.H. Waibel, and P.J. Schenarts, Disparity between resident and faculty surgeons' perceptions of preoperative preparation, intraoperative teaching, and postoperative feedback. J Surg Educ, 2011. 68(6): p. 459-64.
Pugh, C.M., et al., A comparison of faculty and resident perception of resident learning needs in the operating room. J Surg Educ, 2007. 64(5): p. 250-5.
Agha, R.A., Annals of Medicine and Surgery - Educating and Developing Leading Physicians and Surgeons. Ann Med Surg (Lond), 2012. 1: p. 1-6.
Ounounou, E., et al., Nontechnical Skills in Surgery: A Systematic Review of Current Training Modalities. J Surg Educ, 2019. 76(1): p. 14-24.
Rogers, S.O., Jr., et al., Analysis of surgical errors in closed malpractice claims at 4 liability insurers. Surgery, 2006. 140(1): p. 25-33.
Greenberg, C.C., et al., Patterns of communication breakdowns resulting in injury to surgical patients. J Am Coll Surg, 2007. 204(4): p. 533-40.
Ahmed, M., et al., Identifying best practice guidelines for debriefing in surgery: a tri-continental study. Am J Surg, 2012. 203(4): p. 523-9.
Williams, R.G., M.J. Kim, and G.L. Dunnington, Practice Guidelines for Operative Performance Assessments. Ann Surg, 2016. 264(6): p. 934-948.
Williams, R.G., et al., A template for reliable assessment of resident operative performance: assessment intervals, numbers of cases and raters. Surgery, 2012. 152(4): p. 517-24; discussion 524-7.
Sanfey, H., R. Williams, and G. Dunnington, Recognizing residents with a deficiency in operative performance as a step closer to effective remediation. J Am Coll Surg, 2013. 216(1): p. 114-22.
George, B.C., et al., Reliability, validity, and feasibility of the Zwisch scale for the assessment of intraoperative performance. J Surg Educ, 2014. 71(6): p. e90-6.
Bohnen, J.D., et al., The Feasibility of Real-Time Intraoperative Performance Assessment With SIMPL (System for Improving and Measuring Procedural Learning): Early Experience From a Multi-institutional Trial. J Surg Educ, 2016. 73(6): p. e118-e130.
Iwaszkiewicz, M., D.A. Darosa, and D.A. Risucci, Efforts to enhance operating room teaching. J Surg Educ, 2008. 65(6): p. 436-40.
Gardner, A.K., M.D. Timberlake, and B.J. Dunkin, Faculty Development for the Operating Room: An Examination of the Effectiveness of an Intraoperative Teaching Course for Surgeons. Ann Surg, 2019. 269(1): p. 184-190.
About the Authors
Jordan D. Wood, MD, is a PGY-3 resident of general surgery at Southern Illinois School of Medicine in Springfield.
V. Prasad Poola, MBBS, FACS, is an assistant professor and program director of general surgery at Southern Illinois School of Medicine in Springfield.
John D. Mellinger, MD, FACS, is a professor and division chair of general surgery at Southern Illinois School of Medicine in Springfield.