Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
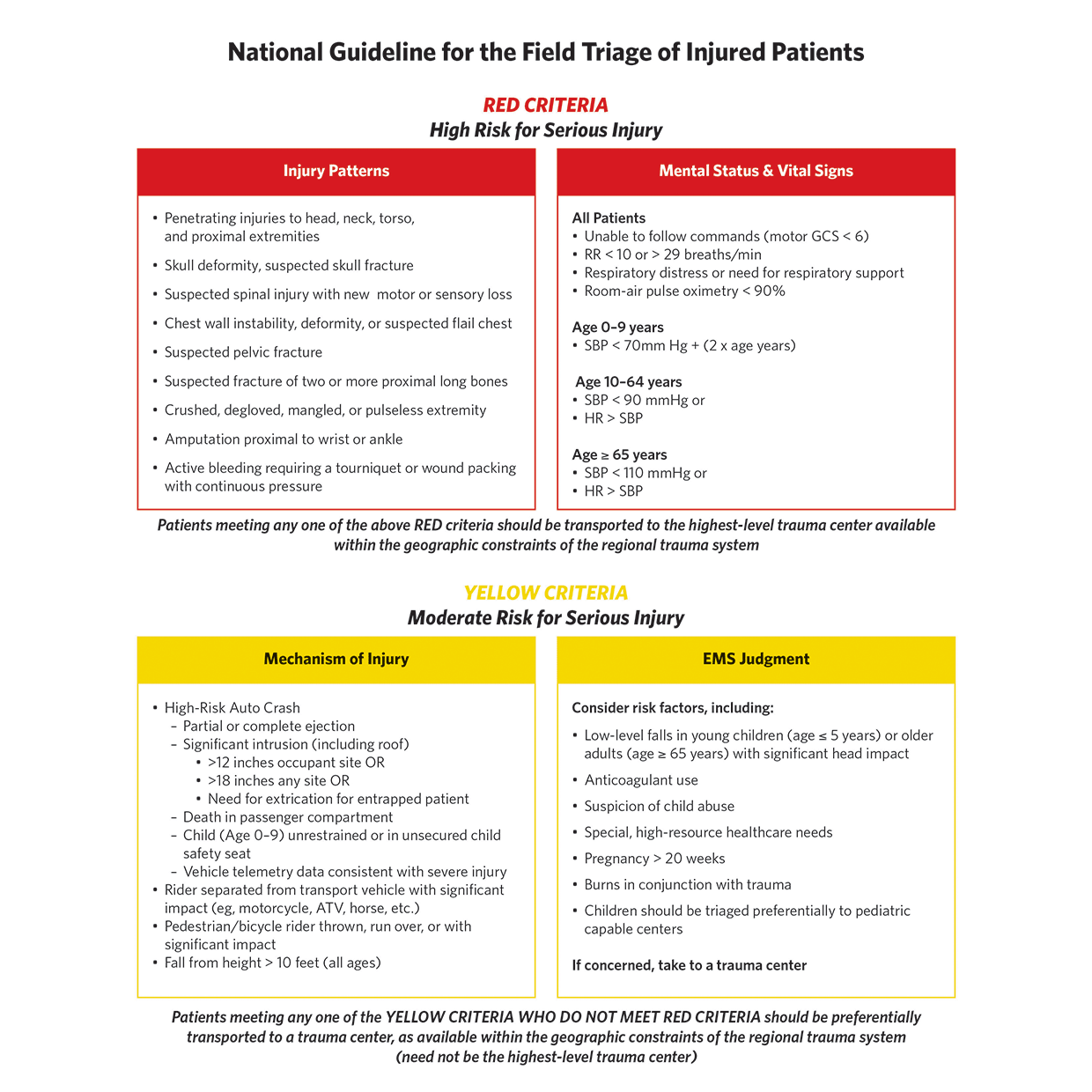
ACS-verified trauma centers save lives and improve long-term outcomes in injured patients, according to a study by Ho and colleagues. These benefits are associated with substantial costs that are incurred to establish and maintain necessary infrastructure.
Data cited in this article showed that the average annual infrastructure cost for a Level 1 trauma center was more than $10 million. Trauma centers are vulnerable to financial stresses because they often treat patients who are uninsured or are covered by government insurance programs that have been subject to recent payment reductions. This study used data from a national dataset and a validated financial vulnerability score to assess financial vulnerability in all ACS-verified trauma centers in California. Key components of the vulnerability score included operating margin, asset-to-liability ratio, days with cash on hand, and time from billing to receipt of payment.
Data from 47 trauma centers for the year 2019 were analyzed. Level 1 centers (44%) had the lowest financial vulnerability; nonetheless one-third of these centers were at high financial risk. Provision of uncompensated or poorly compensated care was a major factor associated with increased financial vulnerability.
Factors associated with low financial vulnerability included larger operating margins, teaching hospital status, and membership in large corporate health systems. The authors concluded that a significant proportion of California trauma centers were financially vulnerable and that the financial vulnerability score was a potentially valuable way to monitor financial status and prevent trauma center closures.
In the editorial that accompanies this article, authors Jessie W. Ho, MD, and Hasan B. Alam, MD, FACS, noted that this study exemplifies the type of research needed to guide decisions about financing not only trauma centers, but other healthcare facilities at risk for closure, such as rural and critical access hospitals. Although the study is limited in that observations are from one state and a significant portion of the trauma centers in the state were excluded from the analysis, the conclusions provided valuable insights. Future studies that use similar analytic methods and include trauma centers and rural and critical access hospitals will be useful.
Could Obese Adolescents Benefit from Broader Access to Bariatric Surgery?
Obesity is a major health issue among adolescents in the US. Although bariatric surgery is known to be an effective means of treating obesity, use of this modality in adolescents remains low. The authors used data from the National Inpatient Sample to analyze trends in frequencies and outcomes of bariatric procedures in patients 9–19 years old over the interval 2015–2018.
The data analysis showed a slight, statistically insignificant increase in procedures during the study interval. Sleeve gastrectomy was the most common operation performed, and most patients were female (76%) ages 17−19 years old. Approximately 48% of the bariatric patients were White; Black and Hispanic patients accounted for 40% of the patient group. Important comorbid conditions included diabetes, hyperlipidemia, non-alcoholic fatty liver disease, hypertension, and sleep apnea. Of note were the observations that no in-hospital mortality was reported, and the overall complication rate was 1.6%.
The authors concluded that bariatric surgery is a safe approach for management of obese adolescent patients and possibly is underused in this age group.
USPSTF Issues Update on Use of Aspirin to Prevent Heart Disease
The recommendations statement and accompanying editorial provided important information for surgeons who are called upon to care for patients at risk for cardiovascular disease. Cardiovascular disease is a major health problem in the US. More than 1.2 million Americans experience a first myocardial infarction or stroke each year, and cardiovascular disease causes 25% of annual deaths.
The US Preventive Services Task Force (USPSTF) has recommended low-dose aspirin for primary prevention of cardiovascular disease and colorectal cancer. Benefits of aspirin come with an increased risk of gastrointestinal bleeding, intracranial hemorrhage, and hemorrhagic stroke. Available data show that long-term low-dose aspirin use increases the risk of GI bleeding by 58% and intracranial bleeding by 31%. Risk factors for bleeding in patients taking low-dose aspirin for primary prevention include older age, male sex, diabetes, history of gastrointestinal disease, liver disease, smoking, and hypertension.
Because the benefits of other therapies such as statins and antihypertensive agents may influence the effectiveness of aspirin, the USPSTF updated its 2016 recommendations for use of aspirin as a primary prevention approach in various age groups. The new recommendations are that patients 40−59 years old with a 10% or greater risk of cardiovascular events over 10 years based on the American College of Cardiology/American Heart Association risk calculator be considered for primary prevention with low-dose aspirin. The decision to treat should be individualized and reached using shared decision-making with each patient.
The USPSTF recommended against initiating aspirin for primary prevention of cardiovascular events in adults 60 years of age and older; evidence was insufficient to support a recommendation for use of aspirin to prevent colorectal cancer. Adoption of these recommendations could optimize prevention of myocardial infarction and stroke.