Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Delivering Difficult Patient Conversations Is a Skill to be Learned, Practiced
Jennifer Bagley, MA
February 8, 2023
15 MinPrintShare
Bookmark
“I’m afraid I have some bad news.”
In medicine, this ominous phrase often serves as a warning, helping patients brace for the impact of difficult news that’s about to be delivered.
“These words let patients know that something is coming. Here I am. I need you to listen. It’s bad,” said Margaret “Gretchen” L. Schwarze, MD, MPP, FACS, a vascular surgeon and the Morgridge Endowed Professor of Vascular Surgery at the University of Wisconsin (UW)-Madison. Dr. Schwarze also is a nationally recognized expert in surgical decision-making, informed consent, advance care planning, and end-of-life care.
Breaking bad news is complex and one of the most sensitive tasks in medicine. Few professional interactions create more anxiety, worry, and deep concern than telling someone painful news.
Sometimes, physicians must let patients and their families know about a severe illness or injury, a cancer diagnosis, a poor prognosis, the occurrence of unwanted and significant side effects, the ineligibility for a clinical trial or transplant, sudden and unexpected death; other times, they’re telling patients the treatment or surgery they thought may work has failed, and it’s time to begin preparing for end-of-life care.
“Bad news” can be defined as information that alters a person’s expectations for the future, is a threat to their physical or mental health, or indicates a risk to an established lifestyle, according to Emily B. Rivet, MD, MBA, FACS, a colon and rectal surgeon at Virginia Commonwealth University (VCU) Health and associate professor at the VCU School of Medicine, both in Richmond. Dr. Rivet, who also is fellowship-trained and board-certified in hospice and palliative medicine, rephrased the definition from a study that examined protocols for breaking bad news.1
“Discussions about difficult medical circumstances can be extremely meaningful and have long-lasting implications,” said Dr. Rivet. “If a patient or caregiver is anxiously awaiting a piece of information, it is best to get right to the point after preparing them for the news by using the warning shot technique.”
Dr. Schwarze recommends that surgeons follow the initial “something is coming” statement with a headline—a very brief statement about what is happening: She needs to go to the operating room. She’s been badly injured. This is a serious infection. The cancer is back.
While physicians notoriously are “explain-aholics” and share a lot of technical details about the disease or treatment, according to Dr. Schwarze, for the purposes of these conversations, the follow-up statement needs to be succinct, but informative—“something for the patients and families to hold onto.”
Dr. Gretchen Schwarze is a nationally recognized expert in surgical decision-making, informed consent, and end-of-life care.
The Emotional Firestorm
After that, the next step is to acknowledge the emotion.
“Can we really have a conversation like this and throw patients and their families into an emotional firestorm without any support?” Dr. Schwarze asked.
She proposes “naming” the emotion: This is terrible. This is so frustrating. It’s so sad that your mother’s health has declined so much.
Patients have every right to be frustrated, Dr. Schwarze continued. “It feels like they’re mad at you. Patients may feel us pushing back because we feel their emotion, and we feel like their emotion is directed at us, so we are defensive. If we supported their emotions, then we could partner with them better. We’d have a much easier relationship, and our patients and their families would trust us more.”
Over the past decade in her research lab, Dr. Schwarze has closely observed what surgeons are saying to patients.
“We use a lot of language around, ‘This is your problem, and this is the operation. I have to fix it.’ We show scans, we draw pictures of the operation, and that makes sense to us. It comes from a good place, but it’s just not very useful to the patients and their families,” she said.
According to Dr. Schwarze, approximately 75% of the time, surgeons do not say what the goal of surgery is (e.g., to help patients live longer or help them feel better). “We forget to tell our patients why we’re doing it and how it will make their lives better.”
These Things Matter, Too
While the words matter, so do their meanings.
Kimberly E. Kopecky, MD, a surgical oncology fellow in the Department of Surgery at The Johns Hopkins University School of Medicine in Baltimore, MD, encourages the use of clear, easy-to-understand language with no euphemisms.
In September 2022, Michelle C. Salazar, MD, MHS, a general surgery resident at the Yale School of Medicine in New Haven, CT, took to Twitter to express the importance of “our patients actually understand[ing] what we’re telling them.” Dr. Salazar described a patient with a worsening cancer burden. The patient had been under the impression that she was getting better because her doctors told her she was “progressing.”
For physicians, progression means that the cancer is getting worse, but the patient understandably perceived the word “progressing” to be favorable. She thought she was making “good progress;” she did not think the disease was progressing.
“Our clinical language isn’t always clear to patients, and this is absolutely essential to recognize,” Dr. Kopecky said.
Nonverbal behavior also matters, she explained. “Being thoughtful and compassionate with how your words land absolutely can be more important than what you actually say. It’s also a skill to know when to stop talking.”
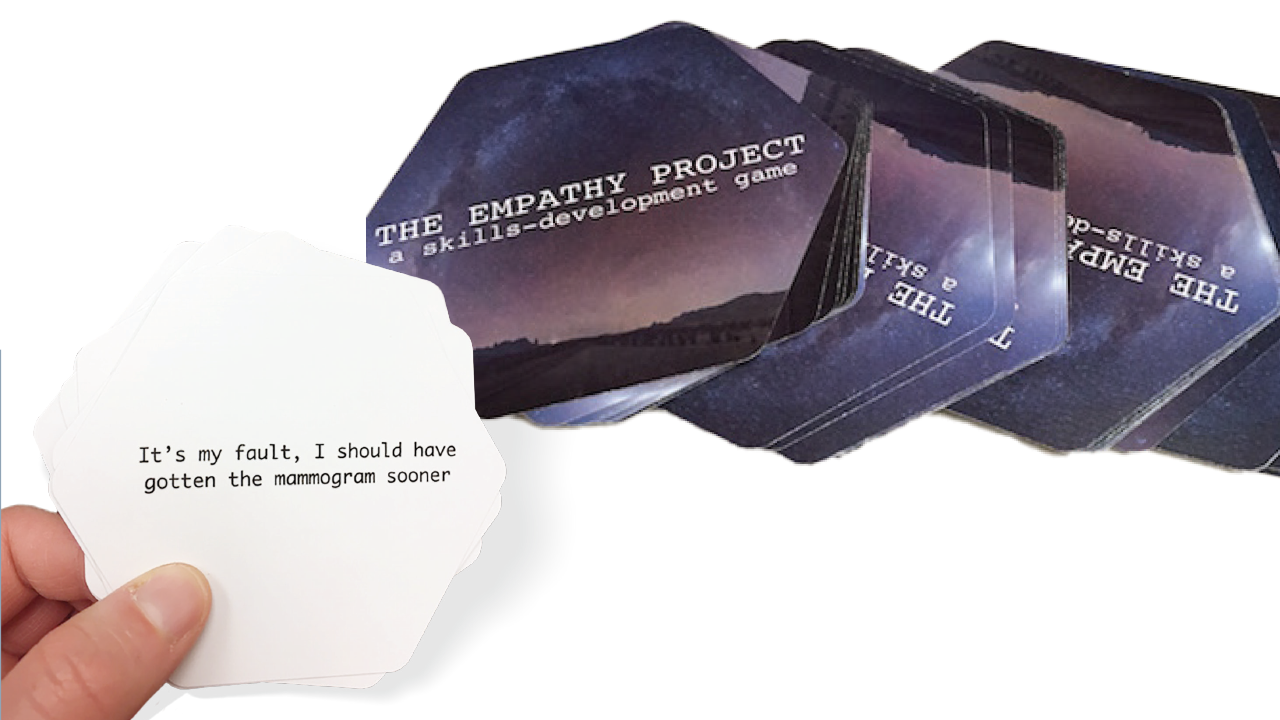
“The Empathy Project” is a card game designed to help physicians hone critical communication skills. The 30 cards feature statements representing commonly expressed emotions such as grief, worry, fear, anger, and guilt.
Learning the Skills
To be a part of patients’ lives in their worst moments is an enormous responsibility.
One study suggests oncologists share bad news as many as 20,000 times over the course of their careers.2 And the physicians who are having these life-changing, critical conversations almost every day are struggling to comfort the sick or dying and their families while agonizing over getting it right.
When they get it right, the consequences can be profound. From a patient perspective, skilled communication from providers has been associated with improved satisfaction, adherence to treatment, better health outcomes, improved recall, and better-quality understanding.3
While this underscores the importance of communication competency, many physicians often feel unprepared to successfully handle such interactions.
Dr. Rivet explained that there is “significant undertraining” for surgeons in communication skills. “It’s time to recognize that these important skills don’t come naturally, and we need to train and measure them with the same degree of seriousness that we teach knot tying, laparoscopic techniques, and other technical abilities,” she said.
A study that examined the sharing of bad news with patients found that 93% of respondents believed delivering grim news is a very important skill, yet only 43% felt they had the proper training to effectively do so.4
Gathering the nuanced clues to make an astute diagnosis, motivating patients to change chronic, detrimental behaviors, and communicating news that changes a person’s expectations about the future are all examples of conversations in medicine that require advanced communication skills, according to Dr. Rivet. “However, until recently, there have been minimal efforts to teach or measure these skills. There has been an assumption that these abilities are innate in successful applicants and aspirants to medical training.”
Nothing could be further from the truth, she said.
Dr. Kopecky said that she doesn’t remember her curriculum on communication training in medical school. Similarly, Dr. Rivet recalled being taught “some communication skills” during her MBA program, but otherwise, she received “very little” communication training.
A 2004 Institute of Medicine report identified basic and complex communication skills as two of the highest priorities for inclusion in medical school curricula.5 The majority of medical schools declare that they now are teaching communication skills within their curricula, though there is tremendous variation in the way and extent to which communication skills are taught and assessed.6
“I wasn’t taught any communication skills. For years, I gave bad news to patients and their families without any skills,” said Dr. Schwarze.
Empathy increasingly is described as one of those learnable skills, yet according to Dr. Kopecky, there are too few effective tools for developing and practicing empathy skills.
In 2016, while hanging out in their cramped workroom lamenting their “lack of grace in dealing with the strong emotions expressed by our patients and their families,” Dr. Kopecky and her coworker, Jasmine A. Hudnall, DO, a hospice and palliative medicine specialist at Gundersen Health System in La Crosse, WI, created a roleplay card game to help hone these critical skills.
They brainstormed about the hardest things they had heard from patients and families, ultimately landing on 25 statements representing a wide variety of expressed emotions, including grief, worry, fear, anger, frustration, and guilt.7
“We started playing this game with the residents and medical students on the service and even the attendings. After a week or so, we decided to look into a way to have the cards printed by a game company because our pieces of paper were deteriorating,” said Dr. Kopecky.
Over the years, medicine has developed its share of protocols for delivering bad news. These widely used frameworks—many of which have been reduced to memorable names or acronyms such as SPIKES, BREAKS, and ABCDE—are designed to make this challenging task easier for physicians and better for patients.
SPIKES, for example, stands for “Setting, Perception, Invitation, Knowledge, Emotion, Summarize.” BREAKS is “Background, Rapport, Exploring, Announce, Kindling, Summarize.” ABCDE is “Advance preparation, Build a therapeutic environment/relationship, Communicate well, Deal with patient and family reactions, Encourage and validate emotions.”
While the protocols differ, many of the ideas are the same: Make sure patients understand their condition. Acknowledge emotions and respond with empathy. Listen. Explain options. Summarize what to expect going forward.
Dr. Rivet added that it’s also important to be prepared. “Steady yourself emotionally, think about practical details such as who should be included and where the discussion should take place. Make sure the medical team is aligned about the message. Lastly, remember that you are there to listen and learn at least as much as to inform,” she said.
The Best Case/Worst Case communication tool combines narrative descriptions and a handwritten graphic aid to illustrate treatment choices and engage patients and families.
Best Case/Worst Case
Much like an operation, which surgeons would never “do cold,” these conversations should be planned out as much as possible, “You need to think through what you are going to say before you go in there and just dump your thoughts on people,” Dr. Schwarze said.
One way to do that is to use the Best Case/Worst Case framework, With planning and preparation in mind, Dr. Schwarze and her research team at UW-Madison developed the Best Case/Worst Case tool, which is designed to help surgeons structure challenging treatment conversations. Best Case/Worst Case combines narrative descriptions, called scenario planning, and a handwritten graphic aid to illustrate treatment choices and engage patients and families.
Along with the visual aid, surgeons use stories to describe how patients might experience a range of possible outcomes in the best case, worst case, and most likely scenarios, Dr. Schwarze explained. Each treatment option is depicted by a vertical bar, and the length of the bar represents the range of possible outcomes.
A 2017 study showed that before Best Case/Worst Case training, surgeons described the patient’s problem in conjunction with an operative solution, directed deliberation over options, listed discrete procedural risks, and did not integrate preferences into a treatment recommendation. After training, surgeons using Best Case/Worst Case clearly presented a choice between treatments, described a range of postoperative trajectories including functional decline, and involved patients and families in deliberation.8
For more information on the Best Case/Worst Case communication tool, visit patientpreferences.org.
How Do You Stand the Pain?
“If giving difficult news feels easy, you probably aren’t doing it right.” Dr. Kopecky often thinks of this advice that she received from a close mentor.
While it likely won’t ever get easier, “I certainly think that exposure and practice matter; most people can improve their skills in this realm if they put time and effort into it,” she said.
Dr. Schwarze agreed, while also noting the emotional toll that these almost-daily difficult conversations can have on frontline providers and bearers of bad news. “These conversations will absolutely paralyze you as a surgeon if you can’t figure out your strategy to manage it. If you hold it too close, it will eat you alive. If you push it too far away, you will not be a good surgeon. The trick is putting it right here: I feel it. It hurts. But it’s not getting to me,” she said, pointing to her hand on her outstretched arm.
There’s a story of a palliative care pediatrician in the South who makes house calls, visiting with her young, dying patients, Dr. Schwarze shared. During one of the visits, the mom asks the physician, “How do you stand the pain?”
The pediatrician revealed that when she gets in her car to drive to the next home, she listens to loud, angry music, while allowing tears to run down her face. The idea is that she lets it go through her.9
“She feels it, but she lets it out,” said Dr. Schwarze. “I love the idea that there is some space where you put it, you feel it, but then you let it go through you.”
Jennifer Bagley is Editor-in-Chief of the Bulletin and Senior Manager in the ACS Division of Integrated Communications in Chicago, IL.
References
Narayanan V, Bista B, Koshy C. ‘BREAKS’ protocol for breaking bad news. Indian J Palliat Care. 2010; 16(2):61-65.
Fallowfield L, Lipkin M, Hall A. Teaching senior oncologists communication skills: Results from phase I of a comprehensive longitudinal program in the United Kingdom. J Clin Oncol. 1998;16:1961–1968.
Monden KR, Gentry L, Cox TR. Delivering bad news to patients. Proc (Bayl Univ Med Cent). 2016;29(1):101–102.
Cuff PA, Vanselow NA, Institute of Medicine Committee on Behavioral and Social Sciences in Medical School Curricula, eds. Improving medical education: Enhancing the behavioral and social science content of medical school curricula. Washington, DC: National Academies Press (US), 2004.
Association of American Medical Colleges, Task Force on Spirituality, Cultural Issues, and End of Life Care. Contemporary issues in medicine: Communication in medicine (Report III of the medical school objectives project). Available at: https://www.aamc.org/media/24236/download. Accessed January 17, 2023.
Hudnall JA, Kopecky KE. The Empathy Project: A skills-development game innovations in empathy development. J Pain Symptom Manage. 2020;60(1):164-169.
Taylor LJ, Nabozny MJ, Steffens NM, et al. Framework to improve surgeon communication in high-stakes surgical decisions best case/worst case. JAMA Surg. 2017;152(6):531-538.
Bredlau A. Where do you put the pain? JAMA. 2016;315(10):983.